By David Gans · May 11, 2026

Meet your bariatric nutrient needs for lifelong health
Most people leave the hospital after bariatric surgery with a short list of vitamins and a vague sense that they will eventually “get back to normal.” That belief is one of the most dangerous misconceptions in post-op recovery. Your altered anatomy changes how your gut absorbs nutrients permanently, which means your supplement regimen is not a temporary bridge. It is a lifelong commitment, and getting it right protects your bones, your nerves, your blood, and your long-term quality of life.
Table of Contents
- Why bariatric nutrient needs are lifelong
- The ASMBS vitamin and mineral minimums for 2026
- Tailoring supplements by procedure and lab results
- When and how to escalate supplementation: special scenarios
- The role of ongoing surveillance and support
- Why so many patients fall through the cracks, and what really works
- Find the right supplements to support your journey
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Lifelong supplementation is essential | Following ASMBS guidance, vitamin and mineral supplements are needed for life after bariatric surgery. |
| Personalize your nutrient plan | Adjust your doses and supplement choices based on your procedure and regular lab results. |
| Watch for warning signs | Symptoms like fatigue, numbness, or frequent vomiting signal urgent review with your provider. |
| Stay vigilant even years later | Nutrient deficiencies can appear long after surgery, making regular checkups and supplements crucial. |
| Use high-quality, ASMBS-aligned products | Choose trusted, ASMBS-recommended supplements, not generic or gummy vitamins, for best results. |
Why bariatric nutrient needs are lifelong
After gastric bypass, sleeve gastrectomy, or duodenal switch surgery, your digestive tract no longer processes vitamins and minerals the way it used to. The stomach is smaller, stomach acid production drops, and in bypass procedures, food bypasses portions of the small intestine where key nutrients are absorbed. These changes do not reverse over time. They are structural.
What surprises many patients is how gradually deficiencies can develop. You might feel completely fine for the first year or two, then the body catches up with you. Bone density quietly drops. Ferritin levels (stored iron) slip below normal. Serum B12 falls even though you feel okay. By the time symptoms appear, real damage may already be underway.
The risks of unmet micronutrient needs are serious and well documented:
- Bone loss and osteoporosis: Calcium and vitamin D malabsorption accelerates bone breakdown over time
- Anemia: Iron deficiency anemia is one of the most common long-term complications, especially in premenopausal women
- Peripheral neuropathy: Low thiamine and B12 can cause tingling, numbness, and nerve damage
- Vision problems: Vitamin A deficiency, more common after duodenal switch, can affect night vision
- Kidney stones: Oxalate absorption increases after gastric bypass, raising stone risk without adequate calcium intake
The common vitamin deficiencies seen in long-term post-op patients are not rare edge cases. They are predictable, preventable, and manageable with the right supplementation plan.
Expert consensus is clear: Supplementation is lifelong and includes a bariatric-specific multivitamin plus targeted micronutrients, not just a standard grocery store supplement. A 2025 systematic review confirms that routine lifelong supplementation and surveillance is the current consensus across expert guidelines.
Labs and clinical follow-up are not optional extras. They are the only way to catch emerging deficiencies before they become irreversible. Your care team, your supplement regimen, and your commitment to monitoring all work together as one system.
The ASMBS vitamin and mineral minimums for 2026
Understanding why you need lifelong supplementation is step one. Knowing exactly what to take is step two. The following table summarizes the current minimum daily targets based on ASMBS-endorsed guidance and expert recommendations in effect for 2026.
| Nutrient | Minimum daily target | Key notes |
|---|---|---|
| Thiamine (B1) | 12 mg | Critical for nerve function; escalate if vomiting |
| Vitamin B12 | 350–500 mcg | Oral or sublingual preferred; adjust to labs |
| Calcium | 1,200–1,500 mg | Citrate form preferred; split into 2–3 doses |
| Vitamin D | Dose to maintain 25 OH vitamin D ≥30 ng/mL | Higher doses often required post-op |
| Iron | 45–60 mg elemental iron | Higher for premenopausal women or those with anemia |
| Folate | 400–800 mcg (800–1,000 mcg for women of childbearing age) | Critical if pregnancy is possible |
| Zinc | 8–22 mg | Monitor; excess zinc can deplete copper |
| Copper | 1–2 mg | Often overlooked; deficiency causes neurological symptoms |
| Vitamin A | 5,000–10,000 IU | Higher for malabsorptive procedures |
A few things stand out here. First, these are minimums, not optimal targets. Many patients, especially those who have had bypass or duodenal switch surgery, require higher doses to maintain healthy blood levels. Second, the form matters. Calcium carbonate, for example, requires stomach acid to absorb and is poorly absorbed after procedures that reduce acid production. Calcium citrate absorbs better in a low-acid environment and is the recommended form for bariatric patients.
Why should you avoid gummy vitamins? Here is a short list of reasons that matter clinically:
- Gummies almost never contain iron, which is one of the most critical nutrients post-op
- Their vitamin D and B12 doses are typically too low to meet bariatric minimums
- Sugar content interferes with weight goals and can trigger dumping syndrome in bypass patients
- Quality control and bioavailability in gummies are generally lower than in capsule or chewable forms
A quality bariatric multivitamin is specifically formulated to meet these elevated minimums in a form your altered gut can absorb. Standard multivitamins from retail stores are formulated for people with intact digestive anatomy and fall well short of what you need.
Pro Tip: Never take calcium and iron supplements at the same time. Calcium significantly blocks iron absorption. Space them at least two hours apart, and take iron with vitamin C to maximize uptake.

Tailoring supplements by procedure and lab results
Not all bariatric procedures carry the same nutrient risks. A sleeve gastrectomy primarily restricts volume, while gastric bypass and duodenal switch also reduce the length of intestine that absorbs nutrients. The more malabsorptive the procedure, the more aggressive the supplementation and monitoring need to be.
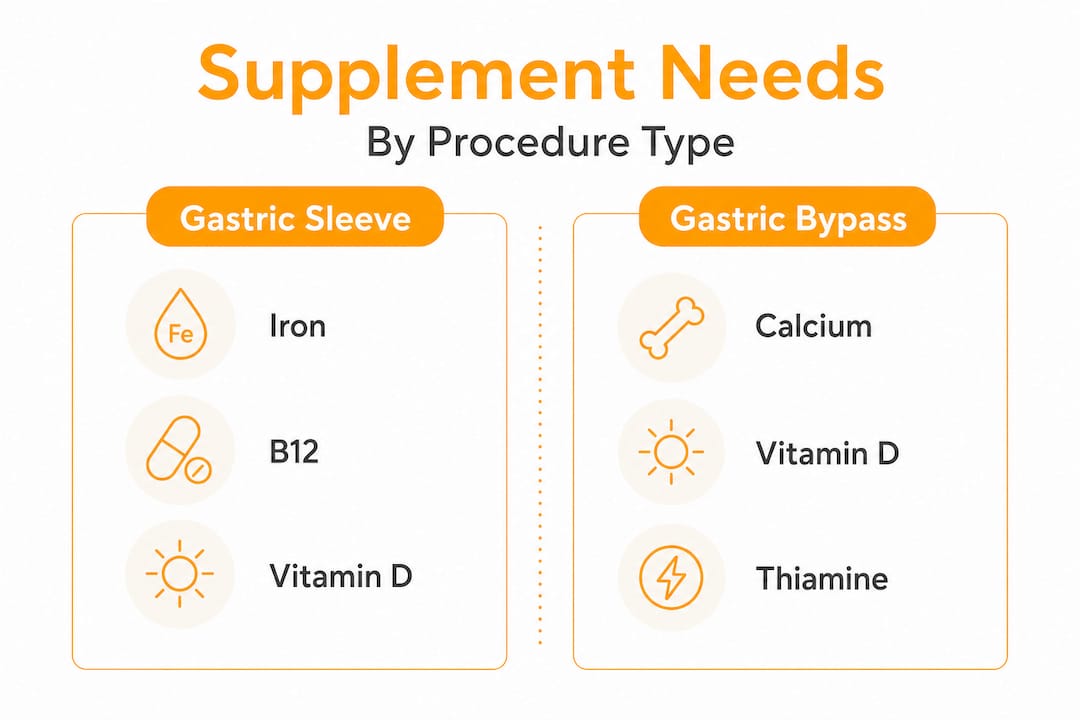
Supplementation should be tailored to the specific type of procedure and adjusted based on ongoing lab results.
| Procedure | Highest nutrient risks | Key adjustments |
|---|---|---|
| Gastric sleeve | Iron, B12, vitamin D, zinc | Standard bariatric multi; monitor annually |
| Gastric bypass (RYGB) | Iron, B12, folate, thiamine, calcium, vitamin D | Higher iron dose; calcium citrate only; B12 sublingual or injection |
| Mini-bypass (OAGB) | Same as RYGB, plus fat-soluble vitamins (A, D, E, K) | Fat-soluble vitamin monitoring critical |
| Duodenal switch (BPD/DS) | All fat-soluble vitamins, iron, calcium, protein | Maximum supplementation; quarterly labs often needed |
Your procedure type gives you a baseline. Your labs tell you where you actually stand. Use both together to build a regimen that fits your body, not just a generic checklist.
Here is a practical framework for tailoring your supplement plan:
- Know your procedure. Confirm with your surgeon whether your surgery was purely restrictive or also malabsorptive. This determines your baseline risk profile.
- Review your labs. Check serum B12, ferritin, 25 OH vitamin D, folate, zinc, copper, and a complete metabolic panel at least once per year, or more often in the first two years post-op.
- Adjust your supplements. Work with your dietitian or bariatric physician to increase doses where levels are low or trending downward. Do not wait for a clinical deficiency to act.
- Repeat monitoring. Set calendar reminders. Life gets busy, and annual lab checks are easy to skip. Treat them like a required maintenance appointment.
Browse procedure-based vitamin guides for more detailed information on what specific procedures require and which products are formulated to meet those demands.
Pro Tip: Symptoms like fatigue, tingling in your hands or feet, vision changes, or hair loss are not “just life after surgery.” They are warning signs that warrant a call to your provider and a lab check, not a wait-and-see approach.
When and how to escalate supplementation: special scenarios
Routine supplementation handles day-to-day needs. But certain situations demand a faster, more aggressive response. Knowing when to escalate is as important as knowing what to take.
Thiamine deficiency is one of the most critical “can’t miss” risks after bariatric surgery. Persistent vomiting, whether from pregnancy, food intolerances, or procedural complications, depletes thiamine rapidly. Unlike most deficiencies that develop slowly, severe thiamine deficiency can cause Wernicke encephalopathy, a neurological emergency, within weeks. If you are vomiting regularly for any reason, thiamine escalation should happen immediately, not after your next scheduled lab.
Signs of B12 deficiency overlap with thiamine: fatigue, brain fog, numbness, and tingling are common to both. Getting labs before you can attribute symptoms to a specific cause is always the right move.
Contact your provider immediately if any of the following apply:
- You have been vomiting multiple times per day for more than 48 hours
- You notice new or worsening numbness or tingling in your hands, feet, or face
- You experience sudden vision changes or difficulty with balance and coordination
- You are pregnant or trying to conceive (folate and iron needs increase significantly)
- You have missed more than two weeks of your regular supplement regimen due to illness, travel, or cost
- Your most recent labs show a value outside the reference range for any key micronutrient
Pro Tip: Never wait for a deficiency to become symptomatic before escalating. Thiamine depletion can cause permanent nerve damage within a matter of weeks. Timely action prevents harm that no supplement can later reverse.
The role of ongoing surveillance and support
Supplementation without monitoring is essentially winging it. You might be fine. Or you might be quietly depleting nutrients that your labs would have flagged months earlier. The only way to know is to test.
Deficiencies, notably iron and B12/folate, can emerge or persist years after surgery, even in patients who have been supplementing consistently. Absorption changes, life stressors, dietary shifts, or medication interactions can all disrupt nutrient status long after the initial post-op period.
Ongoing surveillance is not just a safety net. It is how you stay ahead of problems before they affect your health and daily function. A practical approach includes:
- Annual labs at minimum: Ferritin, serum B12, 25 OH vitamin D, folate, zinc, copper, complete metabolic panel, and CBC (complete blood count) should be reviewed every year
- More frequent testing in high-risk periods: Pregnancy, illness, major dietary changes, new medications, or any new symptoms warrant earlier testing
- Regular dietitian check-ins: A registered dietitian with bariatric experience can review your labs in context and help adjust your regimen accordingly
- Symptom tracking: Keep a simple log of energy levels, hair changes, mood, and any new physical symptoms between appointments
- Medication review: Some medications, including metformin, proton pump inhibitors, and certain antibiotics, deplete specific nutrients and may require additional supplementation
Vitamin D optimization deserves a specific mention here. Beyond bone health, adequate 25 OH vitamin D levels are linked to immune function, muscle strength, and mood regulation. Research increasingly connects vitamin D and mental health, with low levels associated with depressive symptoms. Given that mood challenges are common in the post-op period, this is one micronutrient you really do not want to let slip.
The long-term deficiency risks are entirely preventable with consistent supplementation and routine monitoring. That combination is your strongest protection.
Why so many patients fall through the cracks, and what really works
I am David Gans, and I had gastric bypass in January 2024. I lost 231 lbs and consider the surgery one of the best decisions I have ever made. But I will be honest: I did not fully understand the supplement picture right away. Like many people, I thought the heavy-duty supplementing was a short-term thing. I thought once my labs stabilized, I could ease off. That is not how it works.
The reality is that most patients who develop deficiencies years after surgery did not stop caring about their health. They stopped supplements because of cost, because they felt great, because life got complicated, or because someone told them their labs looked fine and they did not need to be so strict. All of those feel like reasonable reasons in the moment.
The uncomfortable truth is that feeling fine is not a reliable indicator of nutritional status. By the time you feel the effects of iron-deficiency anemia or peripheral neuropathy from B12 loss, you have already been deficient for a significant period. Preventive action is always less costly and less painful than corrective treatment.
What actually works is building supplementation into your daily routine the same way you brush your teeth. It is not optional on busy days. It is not something you revisit every few months. It is a daily, non-negotiable habit backed up by annual labs and a care team who knows your history.
Use pill organizers, phone alarms, or subscription delivery to remove friction. A post-op supplement transition guide can help you understand the shift from immediate post-op supplementation to a sustainable, long-term regimen. The goal is not perfection. The goal is consistency over years, not weeks.
Work with your care team as a partner, not just a checkup appointment. Share your full supplement list, ask about drug-nutrient interactions, and bring your lab trends to appointments rather than just the most recent result. That kind of informed, engaged partnership is what separates patients who thrive long-term from those who struggle.
Find the right supplements to support your journey
Understanding your nutrient needs is the foundation. Finding the right products to meet those needs is the practical next step. If you have been relying on a general multivitamin or winging it with whatever is on sale, your labs will eventually tell the story.
At BestBariatricMultivitamins.com, I compare top bariatric vitamins side by side, looking at price per day, iron content, form (capsule, chewable, or dissolvable), and fit for your specific procedure. I also cover calcium specifically, because it is one of the most under-dosed nutrients in post-op patients. If you are not sure whether your current calcium supplement is the right form or dose, start with our best calcium for bariatric patients guide. Every recommendation is grounded in ASMBS guidelines and real patient experience.
Frequently asked questions
Do I really need to take bariatric vitamins forever?
Yes. Current ASMBS guidance states that supplementation after bariatric surgery is a lifelong requirement, not a short-term recovery tool. Your altered anatomy permanently changes how nutrients are absorbed.
What is the minimum recommended vitamin B12 dose for bariatric patients in 2026?
The standard minimum is 350–500 mcg per day, taken orally or sublingually, with adjustments made based on serum B12 lab results and any symptoms you report to your provider.
How often do I need lab checks for vitamin and mineral levels?
At least once annually after your initial post-op follow-up period, and more frequently if you have new symptoms, a high-risk procedure type, or a history of any deficiency.
Should I stop taking multivitamins if my labs look normal?
No. Deficiencies can develop or return years after surgery even with consistent supplementation. Normal labs today are a result of your current regimen, not evidence that you no longer need it.
Recommended
- Smart cost-per-day vitamin comparison for bariatric patients
- Bariatric Vitamin Guides for Bypass and Sleeve Patients
- Bariatric Vitamin Deficiencies: What to Watch For
Find your bariatric multivitamin
Compare 15 products by price, surgery type, and iron content.
Compare 15 multivitamins